Previously: Chapter 1; Chapter 2
Image descriptions can be found under the read more tag.





PAGE 23 TITLE: KICKING AND SCREAMING: A FIBRO SYMPTOM COMPENDIUM
Panel 1: Small circles denote “tender points” on a person’s upper body.
Text: One of fibromyalgia’s main symptoms is all-body pain, usually called “wide-spread pain.” This descriptor has been derided as “vague” by some, but…
Asterisk: See Berenson 2008.
Panel 2: An old-fashioned carnival barker tries to attract a crowd.
Text, continuing from panel 1: …for many, the pain itself can be described in very specific terms. At times, my pain makes me feel like some sort of circus freak from the sideshows of years past.
Speech bubble, carny barker: COME ONE, COME ALL! You won’t believe your eyes when you see…THE GIRL THAT’S ALWAYS HURTING!
Panel 3: A crowd of onlookers stares at Anna, who sits atop a platform and speaks to the crowd. The carny barker continues his routine.
Text: That’s just me, though.
Speech bubble, carny barker: THRILL at her aches and pains, which have NO KNOWN CAUSE!
Speech bubble, Anna: Yo, anyone have any vicodin?
Panel 4: Anna appears covered in long needles as the crowd watches. One guy says “Wow.”
Speech bubble, barker: Gasp as her symptoms morph unpredictably!
Speech bubble, Anna: I call this one the “Suit of Needles.”
Thought bubble, Anna: OW!
Panel 5: Anna’s limbs contort into unnatural shapes.
Speech bubble, barker: WATCH as she becomes…
Speech bubble, Anna: Totally twisted!
Panel 6: Anna turns into a slug-human hybrid.
Speech bubble, barker: MARVEL at her quick change into…
Speech bubble, Anna: I’m not lazy, just sluggish.
Panel 7: Anna, now back in her everyday form, has a thousand-yard stare.
Text: The ironic part is that most of these symptoms are invisible, at least to people other than the person with the illness.
Speech bubble, Anna: Crap.
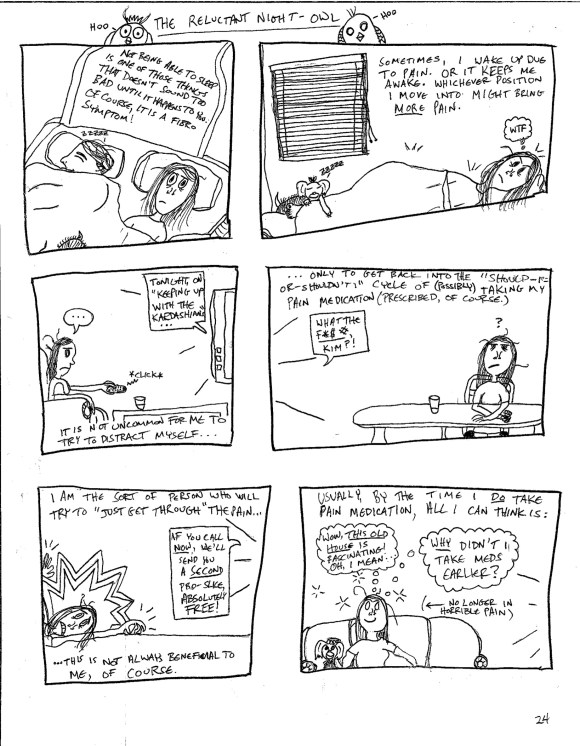
PAGE 24 TITLE: THE RELUCTANT NIGHT-OWL (large owls appear in the page margins.)
Panel 1: Anna and her partner, Liam, are in bed, along with their dog, Winston. Liam is asleep; Anna is not.
Text: Not being able to sleep is one of those things that doesn’t sound too bad until it happens to you. Of course, it is a fibro symptom.
Panel 2: Anna grumbles “WTF” as Winston the dog sleeps soundly atop her.
Text: Sometimes, I wake up due to pain. Or it keeps me awake. Whichever position I move into might bring more pain.
Panel 3: Anna, looking defeated, flips through late-night TV reruns.
Speech bubble, TV announcer: Tonight, on “Keeping Up With the Kardashians…”
Text: It is not uncommon for me to try to distract myself…
Panel 4: Anna sits at her kitchen table with a glass of water, looking either thoughtful or frustrated (or both).
Speech bubble, TV: WHAT THE F**K, KIM?!
Text: …only to get back into the “should I or shouldn’t I” cycle of possibly taking my pain medication (prescribed, of course).
Panel 5: Anna crawls across the floor in pain.
Text: I am the sort of person who will try to “just get through” the pain…this is not always beneficial to me, of course.
Speech bubble, TV infomercial: If you call now, we’ll send you a SECOND Pro-Slice, absolutely FREE!
Panel 6: Anna sits on the couch. She looks relieved.
Text: Usually, by the time I DO take medication, all I can think is…
Thought bubble, Anna: Wow, This Old House is fascinating! Oh, I mean…why didn’t I take meds earlier?
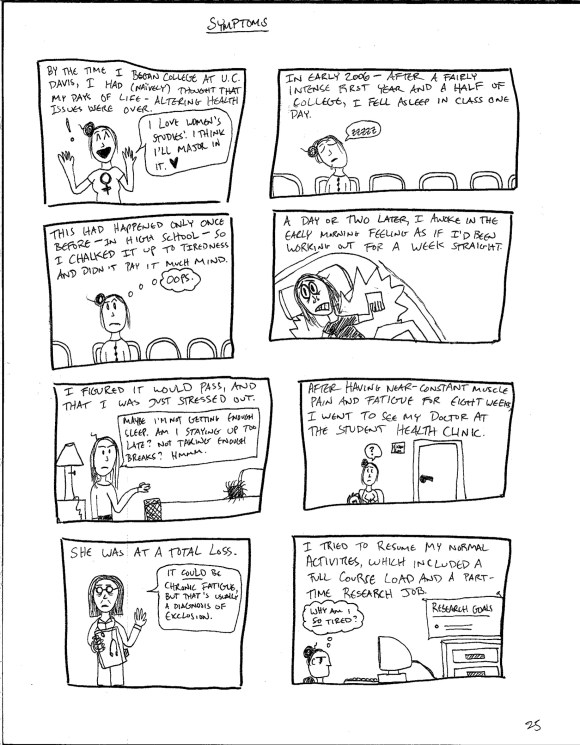
PAGE 25 TITLE: SYMPTOMS
Panel 1: Anna enthusiastically chooses her college major.
Text: By the time I began college at UC Davis, I had (naively) thought that my days of life-altering health issues were over.
Speech bubble, Anna: I love Women’s Studies! I think I’ll major in it.
Panel 2: Anna falls asleep in class.
Text: In early 2006—after a fairly intense first year and a half of college—I fell asleep in class one day.
Panel 3: Anna wakes up in class, embarrassed.
Text: This had happened only once before—in high school—so I chalked it up to tiredness and didn’t pay it much mind.
Thought bubble, Anna: Oops.
Panel 4: Anna wakes up the next morning in considerable pain.
Text: A day or two later, I awoke in the early morning feeling as if I’d been working out for a week straight.
Panel 5: Anna makes her bed as she tries to figure out what is going on with her sudden fatigue.
Text: I figured it would pass, and that I was just stressed out.
Speech bubble, Anna: Maybe I’m not getting enough sleep. Am I staying up too late? Not taking enough breaks? Hmm.
Panel 6: Anna sits in the waiting room at the student health center.
Text: After having near-constant muscle pain and fatigue for eight weeks, I went to see my doctor at the student health clinic.
Panel 7: The doctor speaks to Anna after the exam.
Text: She was at a total loss.
Speech bubble, doctor: It could be Chronic Fatigue, but that’s usually a diagnosis of exclusion.
Panel 8: Anna performs administrative tasks at her part-time job.
Text: I tried to resume my normal activities, which included a full course load and a part-time research job.
Thought bubble, Anna: Why am I so TIRED?
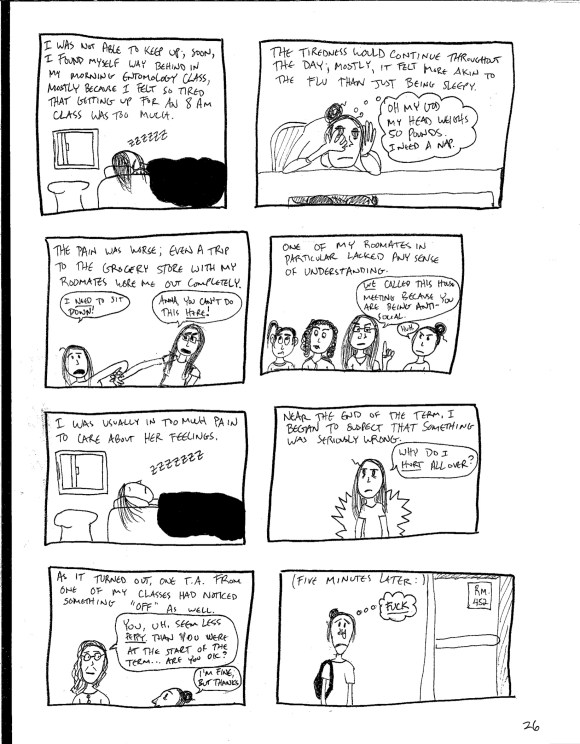
PAGE 26
Panel 1: Anna sleeps in.
Text: I was not able to keep up; soon, I found myself way behind in my morning Entomology class, mostly because I felt so tired that getting up for an 8 AM class was too much.
Panel 2: Anna looks bewildered as she tries to study.
Text: The tiredness would continue throughout the day; it felt more akin to the flu than just being sleepy.
Thought bubble, Anna: Oh my god my head weighs 50 pounds. I need a nap.
Panel 3: Anna tries to sit down at the grocery store as her roommate, Nessa, attempts to stop her from doing so.
Text: The pain was worse; even a trip to the grocery store with my roommates wore me out completely.
Speech bubble, Anna: I need to sit down!
Speech bubble, Nessa: Anna, you can’t do this here!
Panel 4: Nessa has called a “house meeting” with all of the roommates. Fellow roommates Usha and Adela look extremely uncomfortable.
Text: One of my roommates in particular lacked any sense of understanding.
Speech bubble, Nessa: WE called this meeting because you are being antisocial.
Speech bubble, Anna: Huh.
Panel 5: Anna is fast asleep (and snoring) in her room, in the middle of the day.
Text: I was usually in too much pain to care about her feelings.
Panel 6: Anna looks confused as she contemplates the amount of pain she is in.
Text: Near the end of the [school] term, I began to suspect that something was seriously wrong.
Speech bubble, Anna: Why do I hurt all over?
Panel 7: The teaching assistant (T.A.) from one of Anna’s classes takes Anna aside just after class.
Text: As it turned out, one T.A. from one of my classes had noticed something “off” as well.
Speech bubble, T.A.: You seem, uh, less peppy than you were at the start of the term…are you okay?
Speech bubble, Anna: I’m fine, but thanks.
Panel 8: Anna gets emotional as she stands alone outside of the classroom after her meeting with the T.A.
Text: Five minutes later…
Thought bubble, Anna: FUCK.
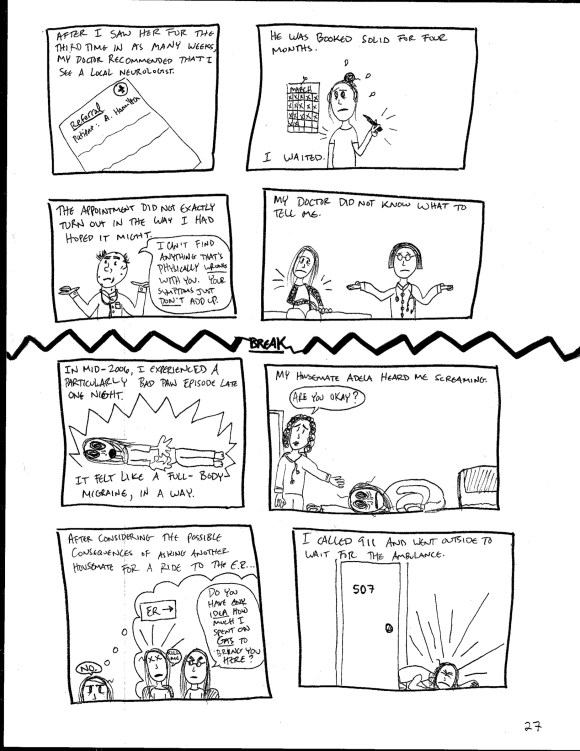
PAGE 27
Panel 1: A referral letter.
Text: After I saw her for the third time in as many weeks, my doctor recommended that I see a local neurologist.
Panel 2: Anna crosses dates off on a wall calendar.
Text: He was booked solid for four months. I waited.
Panel 3: The neurologist tells Anna that he does not know the cause of her symptoms.
Text: The appointment did not turn out in the way that I hoped it might.
Speech bubble, neurologist: I can’t find anything that’s physically wrong with you. Your symptoms just don’t add up.
Panel 4: Anna and her primary care doctor discuss the neurologist’s findings.
Text: My doctor did not know what to tell me.
NEW SECTION TITLE: BREAK
Panel 5: Anna lies on the floor of her apartment in severe pain.
Text: In mid-2006, I experienced a particularly bad pain episode late one night. It felt like a full-body migraine, in a way.
Panel 6: Adela, Anna’s roommate, finds her in fetal position on the floor.
Text: My housemate Adela heard me screaming.
Speech bubble, Adela: Are you okay?
Panel 7: Anna imagines what would happen if she asked Vee to take her to the emergency room; Anna’s thought bubble shows Vee asking “Do you have any idea how much I spent on gas to bring you here?”; imagined Anna squeaks “KILL ME.”
Text: After considering the possible consequences of asking another housemate for a ride to the E.R…
Speech bubble, Anna: NO.
Panel 8: Anna crawls out of the front door of the apartment, with considerable difficulty.
Text: I called 911 and went outside to wait for the ambulance.
PAGE 28
Panel 1: Anna lies on the ground outside, near a bush.
Text: It was nice and cold outside, at least. The EMTs [Emergency Medical Technicians] found me lying under a bush near my apartment.
Panel 2: The EMTs wheel Anna, who is strapped to a wheeled gurney, into an ambulance.
Text: The ambulance crew and the people at the E.R. could not have been nicer. It was weird.
Speech bubble, EMT: We’ll be at the E.R. in no time!
Speech bubble, Anna: Ok.
Panel 3: Anna sits at the intake window at the E.R. and interacts with a staff member.
Text: Even weirder was their apparent willingness to dispense pain medication.
Speech bubble, Anna: EVERYTHING HURTS
Speech bubble, E.R. staff member [cheerfully]: We’ll get you some meds A.S.A.P., okay?
Panel 4: A nurse inserts an intravenous [I.V.] line into Anna’s arm.
Text: I was still fairly squeamish about I.V. needles at that point.
Speech bubble, Anna: Aaaaahh
Speech bubble, nurse: Just a little pinch, here.
Panel 5: Anna looks at the I.V. line, panicked, and then stops panicking suddenly.
Speech bubble, Anna: I WILL NEVER STOP BEING IN PAIN. Wait.
Text: Within a few minutes, something changed.
Panel 6: The medication begins to affect Anna. Several Annas are shown in various stages of happy relief. [Panel has no text.]
Panel 7: Anna realizes that the medication has had an effect.
Thought bubble, Anna: WOW.
Panel 8: Anna is calm and relieved.
Text: For the first time in several months, I felt like I was going to be okay.
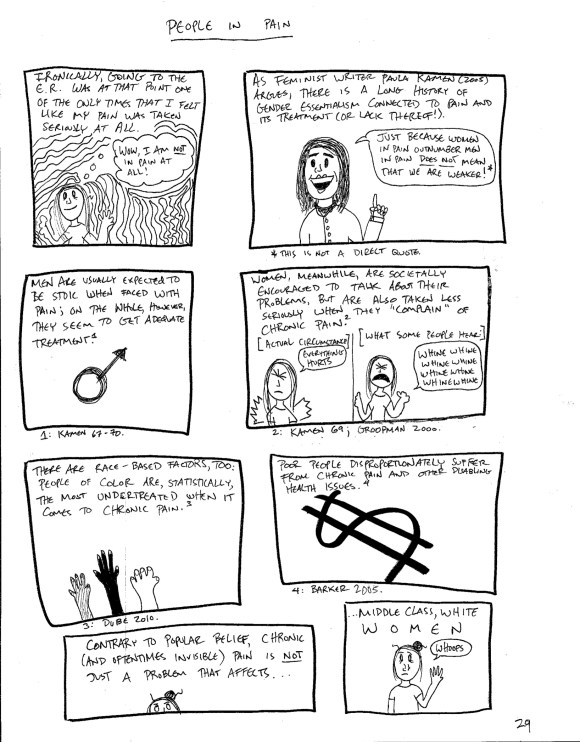
PAGE 29 TITLE: PEOPLE IN PAIN
Panel 1: Anna stands in front of a wavy psychedelic background and is overjoyed at not being in pain.
Text: Ironically, going to the E.R. was at that point one of the only times that I felt like my pain was taken seriously at all.
Thought bubble: Wow, I am not in pain AT ALL!
Panel 2: Author Paula Kamen speaks about gender and pain.
Text: As feminist writer Paula Kamen (2005) argues, there is a long history of gender essentialism connected to pain and its treatment (or lack thereof!).
Speech bubble, Paula: Just because women in pain outnumber men in pain does not mean that we are weaker!
Asterisk: This is not a direct quote.
Panel 3: A “male” symbol stands against a white background.
Text: Men are usually expected to be stoic when faced with pain; on the whole, however, they seem to get adequate treatment.
Footnote: Kamen 67-70.
Panel 4: Two images of Anna experiencing pain. The Anna on the left is labeled “Actual Circumstance,” and the Anna on the right is labeled “What Some People Hear.”
Text: Women, meanwhile, are societally encouraged to talk about their problems, but are also taken less seriously when they “complain” of chronic pain.
Speech bubble, Actual Circumstance Anna: EVERYTHING HURTS.
Speech bubble, What Some People Hear Anna: Whine whine whine whine whine
Footnote: Kamen 69; Groopman 2000.
Panel 5: An abstract image of different hands—black and white—reaching up toward the top of the panel.
Text: There are race-based factors, too: people of color are, statistically, the most undertreated when it comes to chronic pain.
Footnote: Dube 2010.
Panel 6: A large image of a dollar sign dominates the panel.
Text: Poor people disproportionately suffer from chronic pain and other disabling health issues.
Footnote: Barker 2005.
Panel 7: Anna rolls her eyes; only the top half of her face is visible.
Text: Contrary to popular belief, chronic (and oftentimes invisible) pain is not just a problem that affects…
Panel 8: Anna looks worried, as she realizes that her diagnosis of fibromyalgia does not really go against the stereotype of people who have been diagnosed with chronic pain.
Text: …middle-class, white women.
Speech bubble, Anna: Whoops.
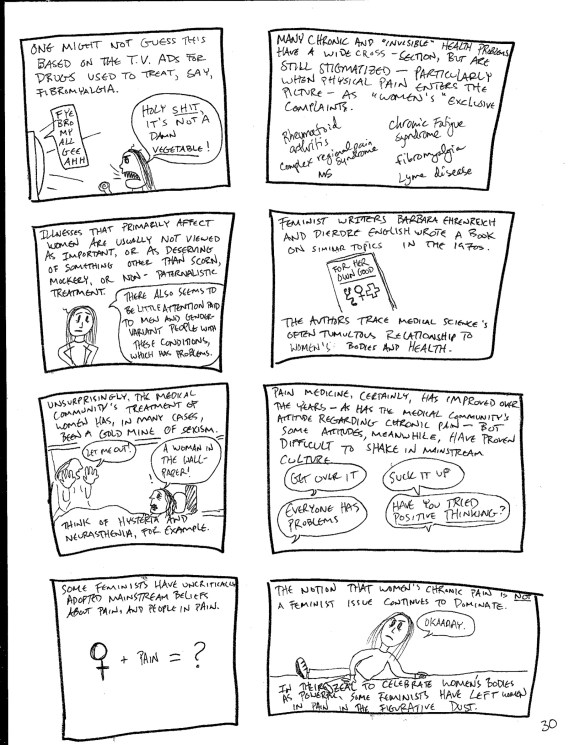
PAGE 30
Panel 1: Anna angrily reacts as she sees an ad for a pharmaceutical product aimed at fibromyalgia patients.
Text: One might not guess this based on the TV ads for drugs used to treat, say, fibromyalgia.
Speech bubble, TV ad: FYE-BRO-MY-ALL-GEE-AH
Speech bubble, Anna: HOLY SHIT, IT’S NOT A DAMN VEGETABLE!
Panel 2: Text featuring the names of various chronic illnesses—rheumatoid arthritis, MS, complex regional pain syndrome, Lyme disease, chronic fatigue syndrome, and fibromyalgia–fills the frame.
Text: Many chronic and “invisible” health problems have a wide cross-section, but are still stigmatized—particularly when physical pain enters the picture—as “women’s” exclusive complaints.
Panel 3: Anna considers some of the issues with the popular imagination defining these illnesses as only being women’s illnesses.
Text: Illnesses that primarily affect women are usually not viewed as important, or as deserving of something other than scorn, mockery, or non-paternalistic treatment.
Speech bubble, Anna: There also seems to be little attention paid to men and gender-variant people with these conditions, which has problems.
Panel 4: Image of the nonfiction book For Her Own Good.
Text: Feminist writers Barbara Ehrenreich and Deirdre English wrote a book on similar topics in the 1970s. The authors trace medical science’s often tumultuous relationship to women’s bodies and health.
Panel 5: Image that references Charlotte Perkins Gilman’s 1892 short story The Yellow Wallpaper; a woman in a bed (enduring the “rest cure” for hysteria) sees a woman in the wallpaper, struggling to get out.
Text: Unsurprisingly, the medical community’s treatment of women has, in many cases, been a gold mine of sexism. Think of hysteria and neurasthenia, for instance.
Speech bubble, protagonist of The Yellow Wallpaper: A woman in the wallpaper!
Speech bubble, woman in the wallpaper: LET ME OUT!
Panel 6: Various speech bubbles, all containing phrases that people with chronic pain commonly hear: Get over it; Suck it up; Everyone has problems; Have you tried POSITIVE THINKING?
Text: Pain medicine, certainly, has improved over the years—as has the medical community’s attitudes regarding chronic pain—but some attitudes, meanwhile, have proven difficult to shake in mainstream culture.
Panel 7: Image of an equation—woman symbol + pain = ?
Text: Some feminists have uncritically adopted mainstream beliefs about pain, and people in pain.
Panel 8: Anna lies on the ground, disgruntled; it looks as if she has fallen and has been left behind by people unseen. She sarcastically and angrily responds to this.
Text: The notion that women’s chronic pain is not a feminist issue continues to dominate.
Bottom text: In their zeal to celebrate women’s bodies as powerful, some feminists have left women in pain in the figurative dust.
Speech bubble, Anna: OKAAAAY.
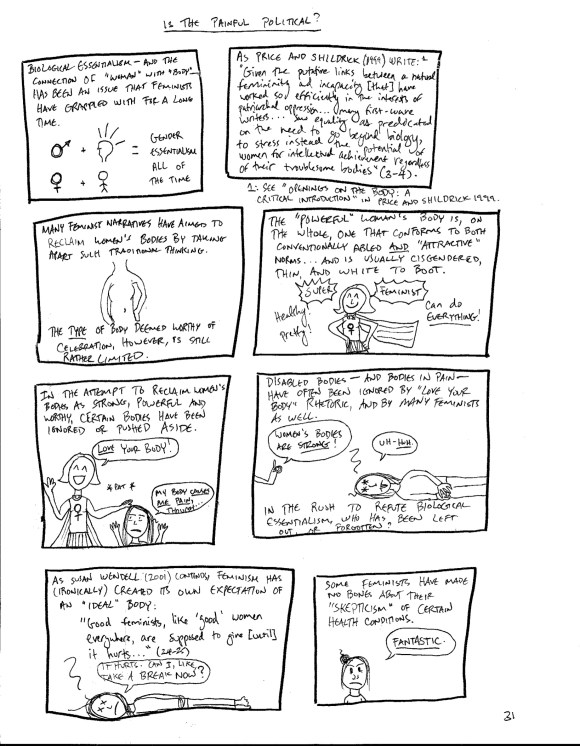
PAGE 31 TITLE: IS THE PAINFUL POLITICAL?
Panel 1: Equations featuring the “male” and “female” symbols associated with brain and body, respectively, equals GENDER ESSENTIALISM ALL OF THE TIME.
Text: Biological essentialism—and the connection of “woman” with “body”—has been an issue that feminists have grappled with for a long time.
Panel 2/Footnote: A quote from Price and Shildrick’s essay “Openings on the Body: A Critical Introduction” (1999).
Text and quote As Price and Shildrick write: “Given the putative links between a natural femininity and incapacity [that] worked so efficiently in the interests of patriarchal oppression…many first-wave writers…saw equality as predicated on the need to go beyond biology, to stress instead the potential of women for intellectual achievement regardless of troublesome bodies (3-4).”
Panel 3: Image of a “standard” body.
Text: Many feminist narratives have aimed to reclaim women’s bodies by taking apart such traditional thinking.
Bottom text: The type of body deemed worthy of celebration, however, is still rather limited.
Panel 4: Image of a Super Feminist who stands proudly while wearing a “female” symbol t-shirt and superhero cape. Text marks her as SUPER FEMINIST! Healthy! Pretty! Can do EVERYTHING!
Text: The “powerful” woman’s body is, on the whole, one that conforms to conventionally abled and “attractive” norms…and is usually cisgendered, thin, and white to boot.
Panel 5: Super Feminist condescendingly pats Anna on the head.
Text: In the attempt to reclaim women’s bodies as strong, powerful, and worthy, certain bodies have been ignored or pushed aside.
Speech bubble, Super Feminist: Love your body!
Speech bubble, Anna: My body causes me pain, though…
Panel 6: Anna lies on the ground in pain as the Super Feminist scolds her.
Text: Disabled bodies—and bodies in pain—have often been ignored by “love your body” rhetoric, and by many feminists as well. In the rush to refute biological essentialism, who has been left out, or forgotten?
Speech bubble, Super Feminist: Women’s bodies are STRONG!
Speech bubble, Anna: Uh-huh.
Panel 7: Anna lies on the ground, in extreme pain.
Text: As Susan Wendell (2001) contends, feminism has created its own expectation of an “ideal” body: “Good feminists, like ‘good’ women everywhere, are supposed to give [until] it hurts…” (24-25)
Speech bubble, Anna: It HURTS. Can I, like, take a break now?
Panel 8: Anna sarcastically responds to feminist “skepticism” of chronic pain conditions.
Text: Some feminists have made no bones about their “skepticism” of certain health conditions.
Speech bubble, Anna: FANTASTIC.
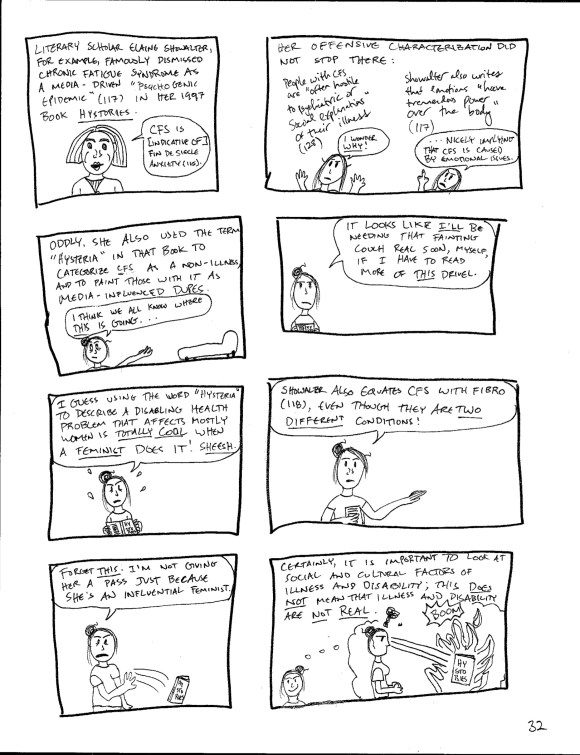
PAGE 32
Panel 1: Elaine Showalter talks about Chronic Fatigue Syndrome.
Text: Literary scholar Elaine Showalter, for example, famously dismissed Chronic Fatigue Syndrome as a media-driven “psychogenic epidemic” (117) in her 1997 book Hystories.
Speech bubble, Elaine Showalter: CFS is [indicative of] fin de siècle anxiety.
Panel 2: Anna takes exception to Showalter’s theories.
Text: Her offensive characterization did not stop there: People with CFS are “often hostile to psychiatric or social explanations” of their illness (128).
Speech bubble, Anna: I wonder WHY.
Text: Showalter also writes that “emotions have tremendous power over the body (117)”
Speech bubble, Anna: …nicely implying that CFS is caused by emotional issues.
Panel 3: Anna gestures to a fainting couch in the background of the panel.
Text: Oddly, she [Showalter] also used the term “hysteria” in that book to categorize CFS as a non-illness, and to paint those with it as media-influenced dupes.
Speech bubble, Anna: I think we all know where this is going.
Panel 4: Anna speaks directly to the reader, book in hand.
Speech bubble, Anna: It looks like I’ll be needing that fainting couch real soon, myself, if I have to read more of this drivel.
Panel 5: Anna continues to speak directly to the viewer.
Speech bubble, Anna: I guess using the word “hysteria” to describe a disabling health problem that affects mostly women is totally cool when a feminist does it! Sheesh.
Panel 6: Anna continues to speak.
Speech bubble, Anna: Showalter also equates CFS with fibro (118), even though they are TWO DIFFERENT CONDITIONS!
Panel 7: Anna throws the book to the side.
Speech bubble, Anna: Forget this. I’m not giving her a pass just because she’s an influential feminist.
Panel 8: Anna smiles as she imagines being able to set Hystories on fire using lasers that shoot from her eyes.
Text: Certainly, it is important to look at social and cultural factors of illness and disability; this does not mean that illness and disability are not real.
PAGE 33 TITLE: THE SOCIAL CONSTRUCTION OF…SOMETHING
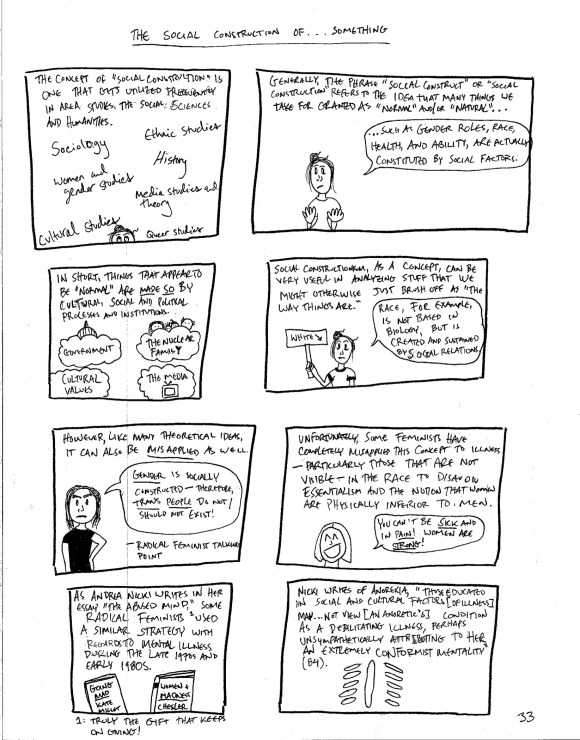
Panel 1: Names of various academic disciplines: sociology, ethnic studies, women’s and gender studies, queer studies, media studies and theory, history, and cultural studies.
Text: The concept of “social construction” is one that gets utilized frequently in area studies, the social sciences and Humanities.
Panel 2: Anna speaks directly to the reader.
Text: Generally, the phrase “social construct” or “social construction” refers to the idea that many things we take for granted as “normal” and/or “natural…
Speech bubble, Anna: …such as gender roles, race, health, and ability, are actually constituted by social factors.
Panel 3: Images that represent abstract concepts: government, the nuclear family, the media, and cultural values.
Text: In short, things that appear to be “normal” are made so by cultural, social, and political processes and institutions.
Panel 4: Anna holds a sign with the word WHITE and an arrow pointing at herself.
Text: Social constructionism, as a concept, can be very useful in analyzing stuff that we might otherwise brush off as “the way things are.”
Speech bubble, Anna: Race, for example, is not based in biology, but is created and sustained by social relations.
Panel 5: Image of an anti-trans radical feminist.
Text: However, like many theoretical ideas, it can also be misapplied as well.
Speech bubble, radical feminist: Gender is socially constructed—therefore, trans people do not/should not exist!
Bottom text: –Radical feminist talking point
Panel 6: A cheerful liberal feminist.
Text: Unfortunately, some feminists have completely misapplied this concept to illness—particularly those that are not visible—in the race to disavow essentialism and the notion that women are physically inferior to men.
Speech bubble, feminist: You can’t be sick and in pain! Women are strong!
Panel 7: Image of two books, Going Mad by Kate Millet and Women and Madness by Phyllis Chessler
Text: As Andrea Nicki writes in her essay “The Abused Mind,” some radical feminists used a similar strategy with regards to mental illness during the late 1970s and early 1980s.
Footnote text: Truly the gift that keeps on giving!
Panel 8: Abstract image of the human ribcage.
Text: Nicki writes of anorexia, “Those educated in social and cultural factors [of illness] may…not view [an anorectic’s] condition as a debilitating illness, perhaps unsympathetically attributing to her an extremely conformist mentality” (84).
PAGE 34
Panel 1: Anna interacts with a fellow feminist.
Text: You can probably guess why this whole “x as only a social construction” business gives me cause for concern.
Speech bubble, feminist: “Fibromyalgia” is a social construction CREATED by the patriarchy to make women think they’re sick!
Speech bubble, Anna: Oh, I knew that was next.
Panel 2: An invisible hand, meant to be the “hand of the patriarchy” referred to in the panel text, pats Anna on the head.
Text: For one thing, it reduces people—women in particular—with chronic, often debilitating conditions like CFS and fibro to agency-free cultural dupes who are easily led by the hand of patriarchy.
Speech bubble, Anna: EVERYTHING HURTS.
Panel 3: Anna sarcastically screams “FETCH ME MY FAINTING COUCH!”
Text: It also suggests—perhaps inadvertently—that by simply having health conditions that feature pain and fatigue as symptoms, we are somehow letting “the sisterhood” down because we are, accidentally, fulfilling stereotypes of women.
Panel 4: An exhausted Anna lies on a fainting couch as someone points at her.
Text: As Nicki points out (85), this sort of reasoning can easily cross the line into blaming ill people for conditions that are not their fault.
Speech bubble, pointing person: Malingerer! You must GET SOMETHING out of being sick.
Speech bubble, Anna (sarcastic): Okay, thanks for clearing that up.
Thought bubble, Anna: FUCK YOU
Panel 5: Various faces parrot mainstream beliefs about people with chronic pain.
Text: When it comes to mainstream ideas about pain, illness, and fatigue, such thinking is not exactly new, liberatory, or feminist.
Speech bubbles: Hysterical, positive thinking, But what if it IS your fault? Whiner, secondary gain, psychosomatic b.s., stupid, psychological problems, shut up, drug addict, ha ha ha, typical attention-seeking female.
Panel 6: s.e. smith, with cat companion.
Text: Writer s.e. smith sums up the wider public opinion on fibromyalgia thusly:
Speech bubble/quote, s.e.: [Fibro] is often assumed to be a specifically “female” complaint, and it’s laden with the double burden of being a “faker’s disease” in the eyes of the American public, who are apparently incredibly knowledgeable about illnesses[…]
Footnote: See smith 2010.
Panel 7: A New York Times headline from January 14, 2008: “Drug Approved. Is Disease Real?” with an arrow denoting “Actual headline”
Text: The media treatment of chronic pain (and conditions that affect women in greater numbers) has not helped.
Footnote: See Thernstrom 2010; Scarry 1988.
Panel 8: A random dudebro wants to share his opinion.
Top text: If anything, it’s made some people who don’t deal with pain believe that they “know” a lot about it from, say, reading a few articles.
Speech bubble, random dudebro: I know all about pain! I read this article in…
Bottom text: …some are NOT shy about sharing.
PAGE 35 TITLE: Diagnosis
Panel 1: Anna reads at her desk.
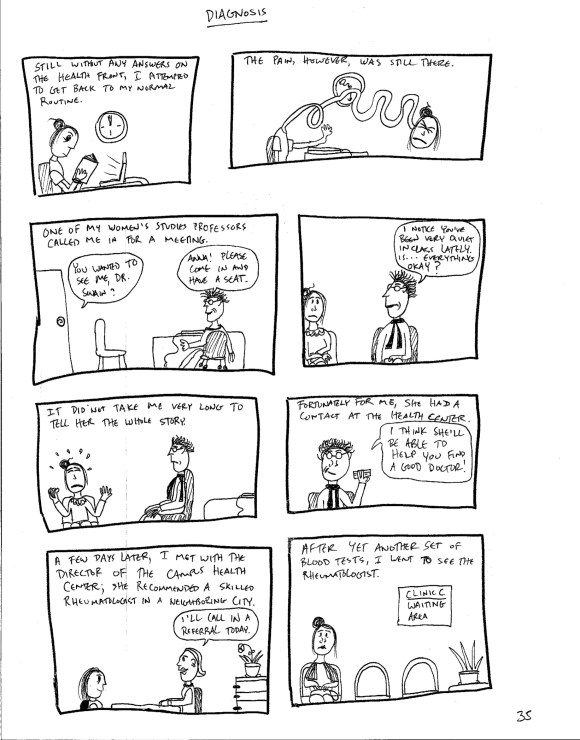
Text: Still without any answers on the health front, I attempted to get back to my normal routine.
Panel 2: Anna imagines her neck painfully stretched into a snake-like form as she grimaces.
Text: The pain, however, was still there.
Panel 3: Anna meets with women’s studies professor Dr. Swain during office hours.
Text: One of my Women’s Studies professors called me in for a meeting.
Speech bubble, Anna: You wanted to see me, Dr. Swain?
Speech bubble, Dr. Swain: Anna! Please come in and have a seat.
Panel 4: Dr. Swain asks Anna what’s going on.
Speech bubble, Dr. Swain: I notice you’ve been very quiet in class lately. Is…everything okay?
Panel 5: An upset Anna tells Dr. Swain about her recent health struggles.
Text: It did not take me very long to tell her the whole story.
Panel 6: Dr. Swain hands Anna a business card.
Text: Fortunately for me, she had a contact at the Health Center.
Speech bubble, Dr. Swain: I think she’ll be able to help you find a good doctor!
Panel 7: Anna meets with Dr. Swain’s contact at the Health Center.
Text: A few days later, I met with the director of the campus Health Center; she recommended a skilled Rheumatologist in a neighboring city.
Speech bubble, Health Center Director: I’ll call in a referral today.
Panel 8: Anna nervously waits at the rheumatologist’s office.
Text: After yet another set of blood tests, I went to see the Rheumatologist.
PAGE 36
Panel 1: The doctor examines Anna.
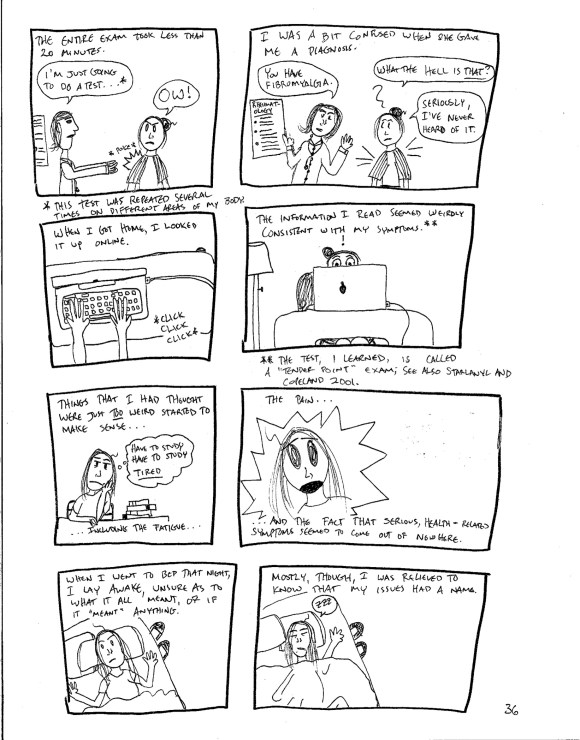
Text: The entire exam took less than 20 minutes.
Speech bubble, doctor: I’m just going to do a test…
Speech bubble, Anna: OW!
Asterisk: This test was repeated on several areas of my body.
Panel 2: The doctor gives Anna a diagnosis.
Text: I was a bit confused when she gave me a diagnosis.
Speech bubble, doctor: You have fibromyalgia.
Speech bubble, Anna: What the hell is that? Seriously, I’ve never heard of it.
Panel 3: Anna’s hands type on a laptop keyboard.
Text: When I got home, I looked it up online.
Panel 4: Anna looks shocked.
Text: The information I read seemed weirdly consistent with my symptoms.
Asterisk: The test, I learned, is called a “tender point” exam; see also Starlanyl and Copeland 2001.
Panel 5: Anna tries not to fall asleep at her desk.
Text: Things that I had thought were just too weird started to make sense…including the fatigue…
Thought bubble, Anna: HAVE TO STUDY. HAVE TO STUDY. TIRED
Panel 6: Anna yelps in pain.
Text: …the pain…and the fact that serious, health-related symptoms seemed to come out of nowhere.
Panel 7: Anna lies in bed and thinks.
Text: When I went to bed that night, I lay awake, unsure as to what it all meant, or if it “meant” anything.
Panel 8: Anna falls asleep and begins to loudly snore.
Text: Mostly, though, I was relieved to know that my issues had a name.
PAGE 37 TITLE: Navel-Gazing
Panel 1: Anna chants “ME ME ME ME ME” at the viewer.
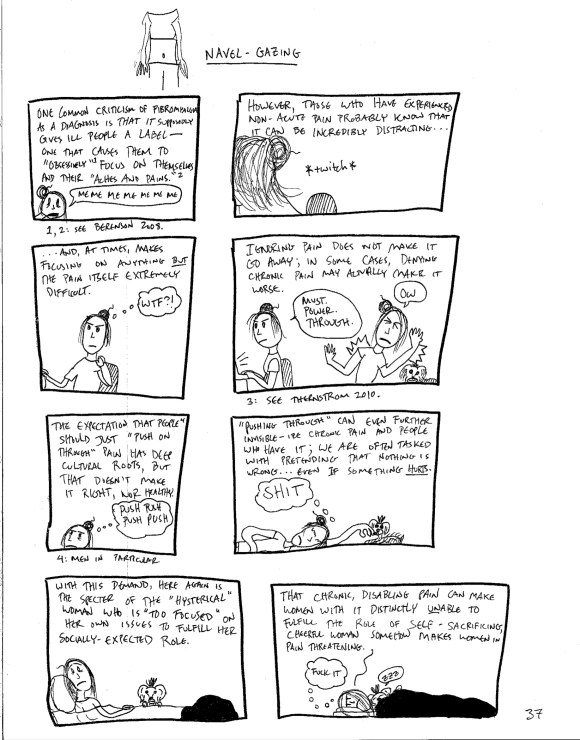
Text: One common criticism of fibromyalgia as a diagnosis is that it supposedly gives ill people a label – one that causes them to “obsessively” focus on themselves and their “aches and pains.”
Footnotes: See Berenson 2008.
Panel 2: We see Anna’s neck twitch as she tries to work.
Text: However, those who have experienced non-acute pain know that it can be incredibly distracting…
Panel 3: Anna massages her neck.
Text: …and, at times, makes focusing on anything BUT the pain itself extremely difficult.
Speech bubble, Anna: WTF?
Panel 4: Anna tries to work through the pain and is unable to do so.
Text: Ignoring pain does not make it go away; in some cases, denying chronic pain may actually make it worse.
Speech bubbles, Anna: Must power through…OW.
Footnote: See Thernstrom 2010.
Panel 5: An exhausted Anna tries to push through her pain.
Text: The expectation that people (footnote) just “push on through” pain has deep cultural roots, but that doesn’t make it right, nor healthy.
Thought bubble, Anna: PUSH PUSH PUSH.
Footnote: Men in particular.
Panel 6: Anna lies on the floor as Winston the Yorkshire Terrier licks her hand.
Text: “Pushing through” can even further invisible-ize chronic pain and people who have it; we are often tasked with pretending that nothing is wrong…even if something hurts.
Thought bubble, Anna: SHIT
Panel 7: Anna and Winston lie in bed. Anna looks unhappy.
Text: With this demand, here again is the specter of the “hysterical” woman who is “too focused” on her own issues to fulfill her socially-expected role.
Panel 8: Anna lies in bed angrily. Winston snores next to her.
Text: That chronic, disabling pain can make women with it distinctly unable to fulfill the role of self-sacrificing, cheerful woman somehow makes women in pain threatening.
Thought bubble, Anna: FUCK IT.
PAGE 38
Panel 1: Anna lugs a single giant rock with great difficulty; the rock metaphorically stands in for Western culture’s expectations of women.
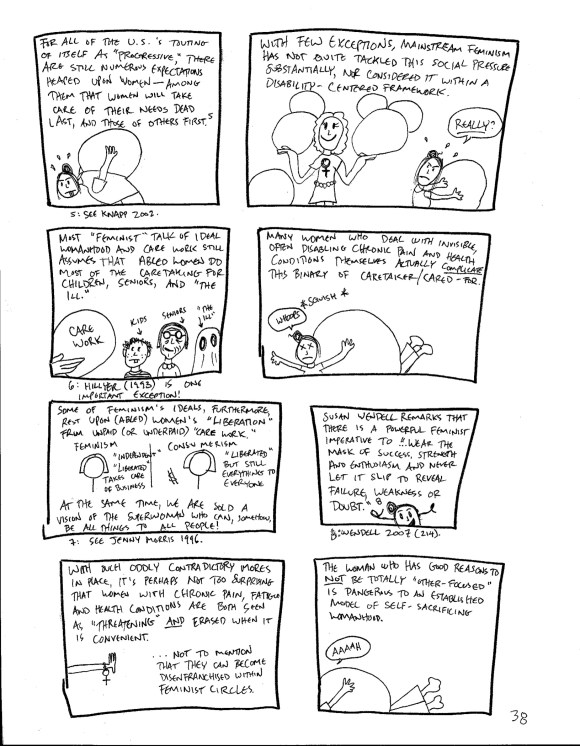
Text: For all of the U.S.’s touting of itself as “progressive,” there are still numerous expectations heaped upon women – among them that women will take care of their [own] needs dead last, and the needs of others first.
Footnote: See Knapp 2002.
Panel 2: Anna sees an able-bodied feminist who balances multiple rocks with ease and with a smile; meanwhile, Anna struggles with her rock.
Text: With few exceptions, mainstream feminism has not quite tackled this social pressure substantially, nor considered it within a disability-centered framework.
Speech bubble, Anna: Really?
Panel 3: A pair of hands holds a rock labeled “care work” as a child, a senior, and a ghost standing in for “the ill” stand in the frame.
Text: Most “feminist” talk of ideal womanhood and care work still assumes that abled women do most of the caretaking for children, seniors, and “the ill.”
Footnote: Hillyer (1993) is one important exception!
Panel 4: The rock that Anna has been struggling to carry rolls over onto her and squishes her.
Text: Many women who deal with invisible, often disabling chronic pain and health conditions themselves actually complicate this binary of caretaker/cared-for.
Speech bubble, Anna: WHOOPS
Panel 5: Image of a woman, contrasting the expectations of ideal feminism and ideal consumerism.
Text: Some of feminism’s ideals, furthermore, rest upon (abled) women’s “liberation” from unpaid (or underpaid) care work. At the same time, we are sold a vision of the superwoman who can, somehow, be all thing
FEMINISM text (left): “Independent,” “liberated,” takes care of business
CONSUMERISM text (right): “Liberated,” but still everything to everyone
Footnote: See Jenny Morris 1996.
Panel 6: A mask decorated to look like Anna’s happy face appears at the bottom of the panel.
Text: Susan Wendell remarks that there is a powerful feminist imperative to “[…] wear the mask of success, strength and enthusiasm and never let it slip to reveal failure, weakness, or doubt.”
Footnote: Wendell 2007 (214).
Panel 7: A hand and wrist wearing a woman-symbol bracelet extends toward the blank space in the rest of the frame, as if prohibiting others from coming in.
Text: With such oddly contradictory mores in place, it’s perhaps not surprising that women with chronic pain, fatigue, and health conditions are both seen as “threatening” and are erased when it is convenient…Not to mention that they can become disenfranchised within feminist circles.
Panel 8: Anna continues to struggle under the rock.
Text: The woman who has good reasons to not be totally “other-focused” is dangerous to an established model of self-sacrificing womanhood.
Speech bubble, Anna: AHHH
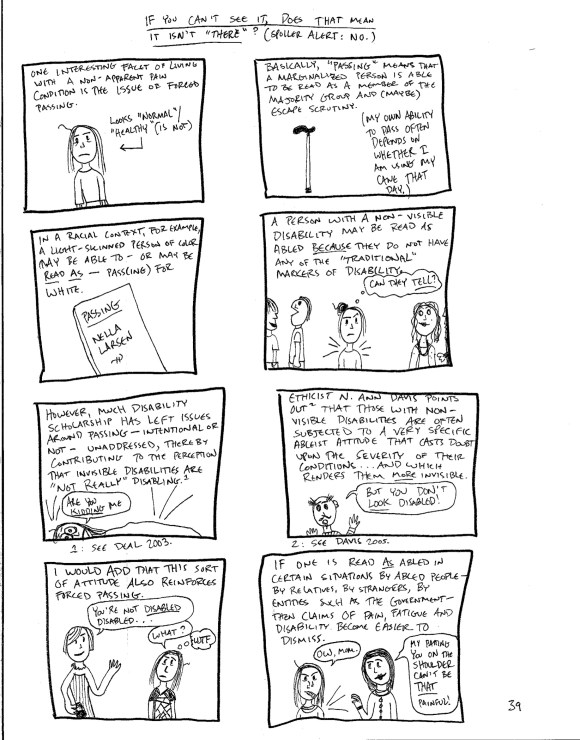
PAGE 39 TITLE: If You Can’t See It, Does That Mean It Isn’t “There?” (Spoiler Alert: No)
Panel 1: Anna stands, looking concerned. An arrow to her right points at her, with the caption “Looks normal/healthy (is not)”
Text: One interesting facet of living with a non-apparent pain condition is the issue of forced passing.
Panel 2: Image of a standard cane.
Text: Basically, “passing” means that a marginalized person is able to be read as a member of the majority group and (maybe) escape scrutiny. (My own ability to pass often depends on whether I am using my cane that day.)
Panel 3: A copy of Nella Larsen’s book Passing.
Text: In a racial context, for example, a light-skinned person of color may be able to – or may be read as – pass(ing) for white.
Panel 4: Anna stands among other people at an event.
Text: A person with a non-visible disability may be read as abled because they do not have any of the “traditional” markers of disability.
Thought bubble, Anna: Can they tell?
Panel 5: Anna lies in bed, obviously in a lot of pain.
Text: However, much disability scholarship has left issues around passing – intentional or not – unaddressed, thereby contributing to the perception that invisible disabilities are “not really” disabling.
Speech bubble, Anna: ARE YOU KIDDING ME
Footnote: See Deal 2003.
Panel 6: A man addresses the viewer.
Text: Ethicist N. Ann Davis points out that those with non-visible disabilities are often subjected to a very specific ableist attitude that casts doubt upon the severity of their conditions…and which renders them more invisible.
Speech bubble, man: But you don’t LOOK disabled!
Footnote: See Davis 2005.
Panel 7: Anna talks to a well-dressed person at a party.
Text: I would add that this attitude
Speech bubble, person: You’re not disabled disabled.
Speech bubble, Anna: What?
Thought bubble, Anna: WTF?
Panel 8: Anna’s mom pats her shoulder, which causes Anna discomfort.
Text: If one is read as abled in certain situations by abled people – by relatives, by strangers, by entities such as the government – then claims of pain, fatigue, and disability become easier to dismiss.
Speech bubble, Anna: Ow, Mom.
Speech bubble, mom: My patting you on the shoulder can’t be that painful!
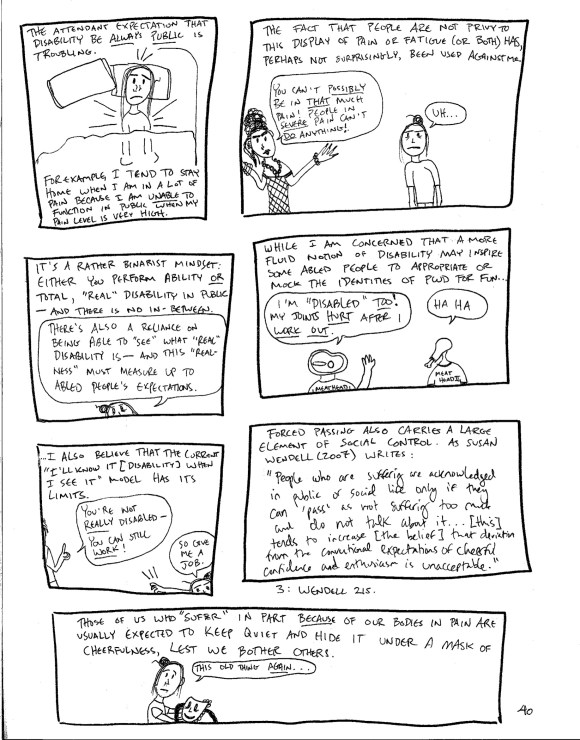
PAGE 40
Panel 1: Anna in bed, in a lot of pain (again).
Text: The attendant expectation that disability be always public is troubling. For example, I tend to stay home when I am in a lot of pain because I am unable to function in public when my pain level is very high.
Panel 2: Anna talks to another person at a party.
Text: The fact that people are not privy to this display of pain or fatigue (or both) has, perhaps not surprisingly, been used against me.
Speech bubble, person: You can’t possibly be in that much pain! People in severe pain can’t do anything!
Speech bubble, Anna: Uh…
Panel 3: Anna speaks directly to the viewer.
Text: It’s a rather binarist mindset: either you perform ability or total, “real” disability in public – and there’s no in-between.
Speech bubble, Anna: There’s also a reliance on being able to “see” what “real” disability is – and this “realness” must measure up to abled people’s expectations.
Panel 4: Two doofuses, Meathead 1 and Meathead 2, talk about how much they hurt after working out.
Text: While I am concerned that a more fluid notion of disability may inspire some abled people to appropriate or mock the identities of PWD for fun…
Speech bubble, Meathead 1: I’m “disabled” too! My joints hurt after I work out.
Speech bubble, Meathead 2: Ha ha
Panel 5: A person scolds Anna, who is crawling through the frame.
Text: …I also believe that the current “I’ll know it [disability] when I see it” model has its limits.
Speech bubble, person: You’re not really disabled – you can still work!
Speech bubble, Anna: Then give me a job.
Panel 6: A quote from Susan Wendell takes up the entire panel.
Text: Forced passing also carries a large element of social control. As Susan Wendell (2007) writes: “People who are suffering are acknowledged in public or social life only if they can ‘pass’ as not suffering too much and do not talk about it…[this] tends to increase [the belief] that deviation from the conventional expectations of cheerful confidence and enthusiasm is unacceptable.”
Footnote: Wendell 215.
Panel 7: Anna looks forlornly at her “happy” mask.
Text: Those of us who “suffer” in part because of our bodies in pain are usually expected to keep quiet and hide it under a mask of cheerfulness, lest we bother others.
Speech bubble, Anna: This old thing again…
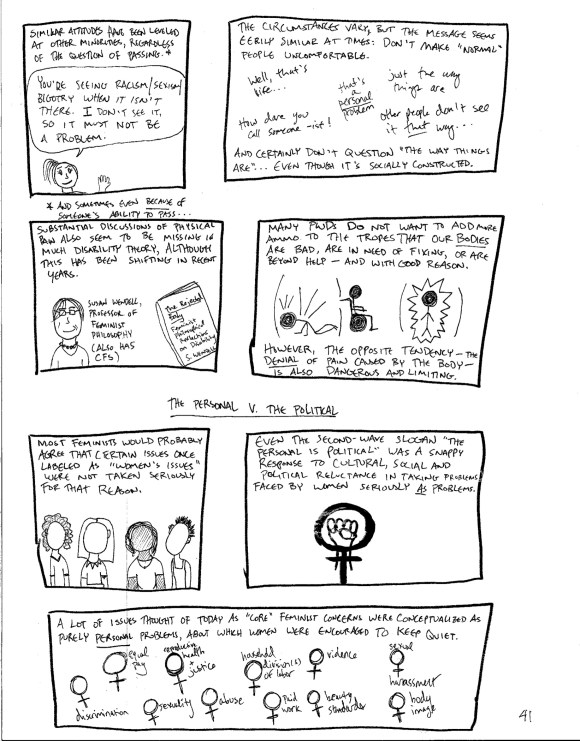
PAGE 41
Panel 1: A young white woman with her hair in a ponytail talks to someone out of frame.
Text, with asterisk: Similar attitudes have been leveled at other minorities, regardless of the question of passing.
Asterisk: And sometimes even because of someone’s ability to pass…
Speech bubble, young woman: You’re seeing racism/sexism/bigotry when it isn’t there. I don’t see it, so it must not be a problem.
Panel 2: Various sayings that people use to minimize bigotry and inequality, including: Well, that’s life! How dare you call someone –ist! Just the way things are! OTHER people don’t see it that way. That’s a personal problem.
Text: The circumstances vary, but the message seems eerily similar at times: Don’t make “normal” people uncomfortable. And certainly don’t question “the way things are…” even though it’s socially constructed.
Panel 3: Feminist philosopher Susan Wendell stands next to a copy of her book The Rejected Body: Feminist Philosophical Reflections on Disability. A caption clarifies that Wendell “also has CFS.”
Text: Substantial discussion of physical pain also seems to be missing in much disability theory, although this has been shifting in recent years.
Panel 4: Three stick-figure PWDs: one kneels on the floor in pain, one sits in a wheelchair, and one stands in abject pain.
Text: Many PWDs do not want to add more ammo to the tropes that our bodies are bad, in need of fixing, or are beyond help – and with good reason. However, the opposite tendency – the denial of pain caused by the body — is also dangerous and limiting.
NEW SECTION TITLE: THE PERSONAL V. THE POLITICAL
Panel 5: Four feminists of various ethnicities.
Text: Most feminists would probably agree that certain issues once labeled as “women’s issues” were not taken seriously for that reason.
Panel 6: Image of a raised fist within the classic “woman” symbol.
Text: Even the second-wave slogan “the personal is political” was a snappy response to cultural, social, and political reluctance in taking problems faced by women seriously as problems.
Panel 7: Listing of various feminist issues that were brought to light during the second and third waves of feminism: discrimination, equal pay, reproductive health and justice, household division(s) of labor, violence, sexual harassment, abuse, sexuality, paid work, beauty standards, body image.
Text: A lot of issues thought of today as “core” feminist concerns were conceptualized as purely personal problems, about which women were encouraged to keep quiet.
PAGE 42
Panel 1: A second-wave consciousness-raising group meets.
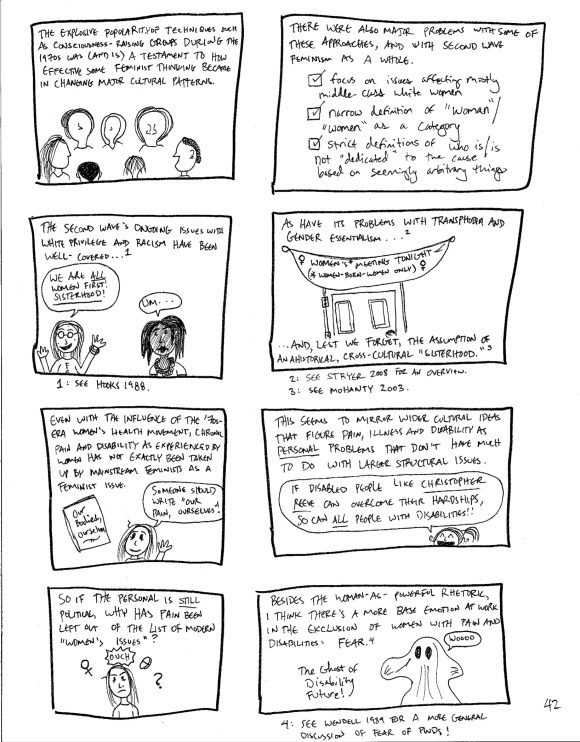
Text: The explosive popularity of techniques such as consciousness-raising groups during the 1970s was (and is) a testament to how effective some feminist thinking became in changing major cultural patterns.
Panel 2: A “checklist” of some issues with second-wave feminism’s approach to women’s liberation: Focus on issues affecting mostly middle-class white women; Narrow definition of “woman”/”women” as a category; Strict definitions of who is/who is not “dedicated” to the cause based on seemingly arbitrary things.
Text: There were also major problems with some of these approaches, and with second-wave feminism as a whole.
Panel 3: A cheerful white woman tells a black woman, “We are all WOMEN first! Sisterhood!” The black woman responds with “Um…”
Text: The second wave’s ongoing issues with white privilege and racism have been well-covered…
Footnote: See hooks 1988.
Panel 4: A banner hanging over a closed door announces a Women’s Meeting TONIGHT, with “women-born-women ONLY” specified in parentheses.
Text: As have its problems with gender essentialism and transphobia…and, lest we forget, the assumption of an ahistorical, cross-cultural “sisterhood.”
Footnotes: See Stryker 2008 for an overview; see Mohanty 2003.
Panel 5: Anna stands next to a copy of Our Bodies, Ourselves.
Text: Even with the influence of the ‘70s-era women’s health movement, chronic pain and disability as experienced by women has not exactly been taken up by mainstream feminists as a feminist issue.
Speech bubble, Anna: Someone should write Our Pain, Ourselves!
Panel 6: A cheerful feminist able-splains disability.
Text: This seems to mirror wider cultural assumptions that figure pain, illness, and disability as personal problems that don’t have much to do with larger structural issues.
Speech bubble, feminist: If disabled people like Christopher Reeve can overcome their hardships, so can ALL people with disabilities!
Panel 7: Anna thinks about the feminist response to chronic pain. The “woman” symbol, the word OUCH, and a large pill circle above her head.
Text: So if the personal is still political, why has pain been left out of the list of modern “women’s issues?”
Panel 8: The “ghost of disability future” appears, saying “Woooo.”
Text: Besides the woman-as-powerful rhetoric, I think there’s a more base emotion at work in the exclusion of women with pain and disabilities: fear.
Footnote: See Wendell 1989 for a more general discussion of fear of PWDs.
PAGE 43
Panel 1: The ghost of disability future says “You have limits” and “WOOOOOO”
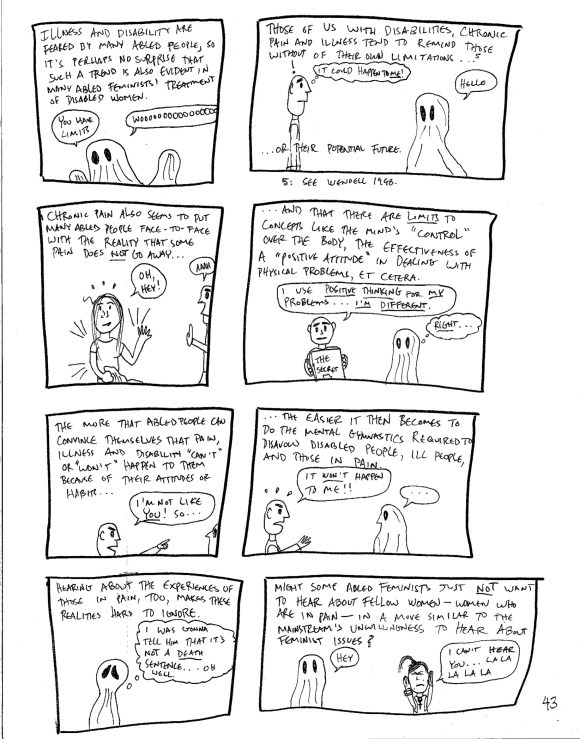
Text: Illness and disability are feared by many abled people, so it’s perhaps no surprise that such a trend is also evident in many abled feminists’ treatment of disabled women.
Panel 2: A man is faced with the ghost of disability future.
Text: Those of us with disabilities, chronic pain and illness tend to remind those without of their own limitations…or their potential future.
Thought bubble, man: It could happen to me!
Speech bubble, ghost: Hello
Footnote: See Wendell 1998.
Panel 3: The ghost removes its sheet to reveal Anna standing there. The man is still ill-at-ease.
Text: Chronic pain also seems to put many abled people face-to-face with the reality that some pain does not go away…
Speech bubble, Anna: Oh, hey!
Speech bubble, man: AHH!
Panel 4: The man holds a large placard promoting new-age book The Secret as the ghost looks on.
Text: …And that there are limits to concepts like the mind’s “control” over the body, the effectiveness of a “positive attitude” in dealing with physical problems, et cetera.
Speech bubble, man: I use positive thinking for my problems…I’m different.
Thought bubble, ghost: Right…
Panel 5: The man turns angrily toward the ghost.
Text: The more that abled people can convince themselves that pain, illness, and disability “can’t” or “won’t” happen to them because of their attitudes or habits…
Speech bubble, man: I’m NOT like you! So…
Panel 6: The man continues angrily addressing the ghost.
Text: …the easier it then becomes to do the mental gymnastics required to disavow disabled people, ill people, and those in pain.
Speech bubble, man (continued from panel 5): It WON’T happen to me!
Panel 7: The ghost, left alone, looks into the distance.
Text: Hearing about the experiences of those in pain, too, makes these realities hard to ignore.
Thought bubble, ghost: I was gonna tell him that it’s NOT a death sentence…oh well.
Panel 8: A feminist puts her hands up to her ears as the ghost approaches her.
Text: Might some abled feminists just not want to hear about fellow women—women who are in pain—in a move similar to the mainstream’s unwillingness to hear about feminist issues?
Speech bubble, ghost: Hey
Speech bubble, feminist: I CAN’T HEAR YOU, LA LA LA LA LA
PAGE 44
NEW SECTION TITLE: PAINFUL LIMITS: ESSENTIALISM, DISABILITY THEORY, AND PAIN
Panel 1: Image of a raised fist reflected in a wheelchair’s wheel.
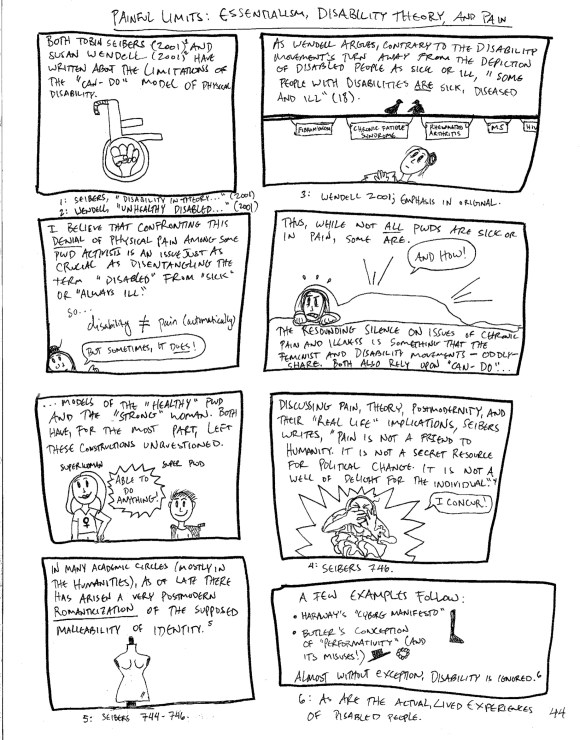
Text: Both Tobin Seibers (2001) and Susan Wendell (2001) have written about the limitations of the “can-do” model of physical disability.
Footnotes: Seibers, “Disability in Theory…” (2001); Wendell, “Unhealthy Disabled…” (2001).
Panel 2: Anna stands beneath a wire, on which she has hung the names of several illnesses/disabilities: fibromyalgia, chronic fatigue syndrome, rheumatoid arthritis, MS, HIV. Two small birds sit on the wire.
Text: As Wendell argues, contrary to the disability movement’s turn away from the depiction of disabled people as sick or ill, “some people with disabilities are sick, diseased and ill” (18).
Footnote: Wendell, 2001; emphasis in original.
Panel 3: Anna addresses the reader, referring to the text that reads disability =/= pain (automatically).
Text: I believe that confronting this denial of physical pain among disability activists is just as crucial as disentangling the term “disabled” from “sick” or “always ill.”
Disability =/= pain (automatically)
Speech bubble, Anna: But sometimes, it does!
Panel 4: Under a blanket, Anna grits her teeth as she has an attack of pain.
Text: Thus, while not all PWDs are sick or in pain, some are. The resounding silence on issues of chronic pain and illness is something that the feminist and disability movements—oddly—share. Both also rely upon “can-do…”
Speech bubble, Anna: And HOW!
Panel 5: A “super” woman and a “super” PWD stand side-by-side. A text burst labels them as “ABLE TO DO ANYTHING!”
Text, continued from panel 4: …models of the “healthy” PWD and “strong” woman. Both have, for the most part, left these constructions unquestioned.
Panel 6: Curled into fetal position, Anna continues to struggle with her pain.
Text: Discussing pain theory, postmodernity, and their “real life” implications, Seibers writes, “Pain is not a friend to humanity. It is not a secret resource for political change. It is not a well of delight for the individual.”
Speech bubble, Anna: I concur!
Footnote: Seibers 746.
Panel 7: Image of a woman’s dress form.
Text: In many academic circles (mostly in the Humanities), as of late there has arisen a very postmodern romanticization of the supposed malleability of identity.
Footnote: Seibers 744-746.
Panel 8: Image of accessories—a necklace, a boot, and a hat.
Text: A few examples follow: Haraway’s “A Cyborg Manifesto,” Butler’s conception of “performativity” (and its misuses!). Almost without exception, disability is ignored.
Footnote: As are the actual, lived experiences of disabled people.
PAGE 45
Panel 1: A group of people are having fun in a room; one dances in a feather boa and yells the word “PERFORMATIVITY!” for seemingly no reason. Anna looks in on the festivities from outside.
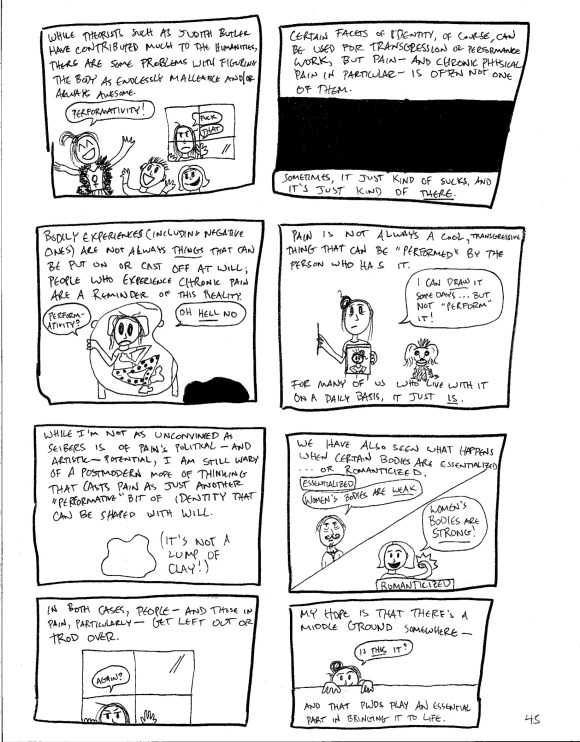
Text: While theorists such as Judith Butler have contributed much to the Humanities, there are some problems with figuring the body as endlessly malleable and/or always awesome.
Speech bubble, Anna: FUCK THAT
Panel 2: A dark void space.
Text: Certain facets of identity, of course, can be used for transgression or performance work, but pain—and chronic physical pain in particular—is often not one of them. Sometimes, it just kind of sucks, and it’s just kind of there.
Panel 3: Anna is bedridden due to pain, in an uncomfortable pose that recalls Francis Bacon’s 1966 painting Lying Figure.
Text: Bodily experiences (including negative ones) are not always things that can be put on or cast off at will; people who experience chronic pain are a reminder of this reality.
Speech bubble, Anna: Performativity? Oh, HELL NO.
Panel 4: Anna, accompanied by her dog, Winston, draws a self-portrait.
Text: Pain is not always a cool, transgressive thing that can be “performed” by the person who has it. For many of us who live with it on a daily basis, it just is.
Speech bubble, Anna: I can draw it some days…but not “perform” it!
Panel 5: Line drawing of a lump of clay.
Text: While I’m not as unconvinced as Seibers is of pain’s political—and artistic—potential, I am still wary of a postmodern mode of thinking that casts pain as just another “performative” bit of identity that can be shaped at will.
Parenthetical text: It’s not a lump of clay!
Panel 6: An old-fashioned doctor with an elaborate mustache and a feminist stand side-by-side in a split panel; they are labeled “Essentialized” and “Romanticized,” respectively.
Text: We have also seen what happens when certain bodies are essentialized…or romanticized.
Speech bubble, doctor: Women’s bodies are WEAK.
Speech bubble, feminist: Women’s bodies are STRONG!
Panel 7: Anna looks through the same window as in panel 1.
Text: In both cases, people—and those in pain, in particular—get left out or trod over.
Speech bubble, Anna: Again?
Panel 8: Anna crawls on the “middle ground,” looking for a more nuanced understanding of women in chronic pain.
Text: My hope is that there’s a middle ground somewhere—and that PWDs play an essential part of bringing it to life.
Speech bubble, Anna: Is this it?
PAGE 46
NEW SECTION TITLE: THE WAY THE WHOLE THING ENDS
Asterisk: With apologies to Gillian Welch for using the title of one of her songs.
Panel 1: Anna sits at her desk drawing.
Text: I have always been terrible at writing conclusions.
Speech bubble, Anna: How am I going to illustrate THAT?
Panel 2: Anna, bewildered, is surrounded by huge phrases commonly used as part of concluding remarks: In the final analysis; in summary; finally; in the future; overall; in this essay, I have argued; this paper has examined; ultimately; and so.
Text: Conclusions have, in fact, been the bane of my writerly existence ever since I could pick up a pencil.
Speech bubble, Anna: I HATE all of these!
Panel 3: Young Anna tries to think of a punch line to a traditional four-panel comic.
Text: Back when I started making comics—at around age 10—I couldn’t stand having to end strips with a punch line!
Panel 4: Anna sits in her living room, reading a book.
Text: The appeal of creative work was—and still is—about the meaty parts of a story, not its end. (Very often, I find that I hate finishing books because the literary amazingness comes to an end!)
Thought bubble, Anna: Nooo…the last ten pages!
Panel 5: Anna sits on her living room chair, deep in thought. Various rough comic pages are tacked onto the wall behind her.
Text: Besides, having to tie up all of a story’s “ends” can feel forced at times.
Thought bubble, Anna: Hmmm.
Panel 6: Anna holds hands with her partner, Liam, a white man with brown hair who wears a pi symbol t-shirt; a small heart symbol is in the space between them. Winston the dog stands nearby, surrounded by flies.
Text: A lot of things have changed since my diagnosis in 2007. Later that year, I met my partner, Liam, on a dating website. (We are still together!)
Panel 7: Anna excitedly screams “HONORS!” while throwing her hands into the air.
Text: I also decided to write an honors thesis for my B.A. [Bachelor of Arts] degree in Women’s Studies.
Panel 8: Anna reads and takes notes for her thesis project in bed. Framed photos and a Tori Amos poster hang on the walls next to her. Winston relaxes next to her feet.
Text: It was a huge undertaking, but it did give me something to focus on other than pain…even if I did do most of it in bed!
PAGE 47
Panel 1: Anna excitedly rushes into her thesis adviser’s office to show off a recently acquired research tool.
Text: It also helped that I was enthusiastic about my chosen subject—the Heaven’s Gate cult, masculinity, and media representation.
Speech bubble, Anna: I have a DVD of thirteen straight hours of HG’s recruitment videos! OH MY GOD.
Speech bubble, Luz (thesis adviser): I’m glad you’re so excited!
Asterisk: Comes with the documentary “Heaven’s Gate: The Day After” (Oneworld Films, 1999).
Panel 2: Anna stands next to a grouping of different “hats” meant to represent the various hats she wears as a student: college student (mortarboard), writing tutor (a trilby/pork pie hybrid with a pencil stuck in one end), feminist (a beanie with the “woman” symbol on it), writer (a plain cap with an exclamation point on it).
Text: Even though I couldn’t handle a full course load with fibro, knowing what I was dealing with made it easier to manage wearing various hats.
Panel 3: Anna lies in bed, in pain, as Liam and Winston comfort her.
Text: Of course, I had—and still had—days where wearing any “hat” other than one befitting a person in pain was impossible.
Speech bubble, Anna: I should be doing more!
Speech bubble, Liam: But you are in pain. It’s okay not to do things when you hurt!
Panel 4: Anna stands under a smiling sun as an empty wheelchair flies across the sky, leaving a rainbow in its wake. Clouds at the other end of the rainbow are labeled with triumph of the human spirit, positive, heartwarming, beauty, inspirational.
Text: It’s an unfortunate result of the “inspirational PWD” figure that so many abled people expect disability narratives to have an “uplifting” ending of some kind.
Speech bubble, Anna: WTF!
Panel 5: Anna stands smiling as she holds a happy rain cloud on a string.
Text: I hate that shit.
Panel 6: Anna addresses the reader directly.
Text: Some might say that I am just jealous of those who can fit their stories into a stock narrative, with appropriately uplifting “beginning,” “middle,” and “end” parts. In some ways, they are (or would be) correct.
Speech bubble, Anna: This action of “fitting” also sometimes reduces nuance and complexity!
Panel 7: Anna looks up at the happy cloud as it passes by.
Text: Chronic pain, by definition, does not end. It just goes on!
Speech bubble, Anna: I guess it can be likened to a cloud that’s always there…
Panel 8: Anna gets out her umbrella as the happy cloud begins to rain droplets.
Text: My fibro has no ending, no inspirational lesson with which I can neatly wrap things up (and perhaps provide the reader with a warm n’ fuzzy feeling, too!).
Speech bubble, cloud: HEY!
Speech bubble, Anna: If we’re going with the weather metaphor…sometimes it rains, sometimes it doesn’t.
PAGE 48
Panel 1: A divided panel shows Anna’s left leg and her swollen face and neck.
Text: The CP does not end. The allergic reactions do not, either.
Footnote: I still get them [allergic reactions] out of nowhere. Fun.
Panel 2: A divided panel shows Anna looking at a pill bottle, then, 30 minutes later (labeled in panel) sitting on the couch with a happy facial expression.
Text: I do get temporary respite from the pain on occasion, thanks to the wonders of prescription drugs…
Thought bubble, Anna: Should I?
Panel 3: Various angry faces and questioning accusations abound as Anna worries, “I am the worst person ever”; the judgment(s) of other people; just take Advil or something; drug-seeking behavior; media concern trolling; guilt; painkiller epidemic; addict; you shouldn’t take those pills…you might get ADDICTED!
Text: …But this often comes with another set of issues.
Footnote: See Parikh 2009.
Panel 4: Anna faces off with another person who is eager to extoll the benefits of positive thinking.
Text: I have commented to close friends that dealing with abled peoples’ responses to my pain is, on the whole, much more difficult than actually dealing with the physical symptoms of fibromyalgia.
Speech bubble, person: Blah blah blah POSITIVE THINKING blah blah blah
Thought bubble, Anna: Could you do me a favor and, like, SHUT UP?
Footnote: For a more thorough explanation of this, see Thernstrom’s The Pain Chronicles (2010).
Panel 5: Anna is tormented by thoughts about her medication use.
Text: Internalized ableism doesn’t help, of course.
Thought bubble, Anna: Does taking this for pain mean I am addicted? I shouldn’t rely on pills so much. Maybe I just need more willpower or something. What must people think of my use of pills?
Spiky speech bubble, Anna: AHHHHH
Panel 6: The words “fibromyalgia,” “anaphylaxis,” and “cerebral palsy” float in the frame, attached to Anna’s fingers by thin threads.
Text: How do you conclude something about a thing that has no conclusion itself?
Speech bubble, Anna: …or multiple things that have no conclusion?
Panel 7: Anna stands in a blank frame and considers the questions brought up by the previous panel.
Text: I suspect it’s a lot like dealing with pain, fatigue, illness, and/or disability. I get this question a lot: “How do you deal with it/go on/get up in the morning/et cetera?”
Text at bottom of frame: You just do.
END OF TEXT
Afterword
A picture may be worth a thousand words because no one word is ever adequate to the excessive expressivity of images.
–Tobin Seibers, from “Words Stare Like a Glass Eye: From Literary to Visual Disability Studies and Back Again” (2004)
One aspect of academic writing, and theory, that has confused me for a long time is the expectation that both will be—and should be—written in a style that is inaccessible to all but a comparatively select few. Part of my reason for choosing a format—the graphic novel—that is not looked at as “serious” was to make some very important theoretical concepts accessible to a non-academic audience. Additionally, my own theoretical project of examining women’s chronic physical pain in contemporary culture relates a lot to my own life experiences, and I have had trouble writing about these experiences “academically enough.”
The potential (and very likely, if we want to be honest) status of my project as “not academic enough” concerns me, to be sure. However, I have tried to write and theorize about my experiences with disability in a more “traditional” format for years, and I have had a nagging suspicion that only writing about these experiences at length leaves something out. With one exception, the often overly formal style of academic writing has, by and large, not worked in my favor. I have written many short-form pieces about disability intended for a general audience; however, my other entrees into theorizing disability in a more academic-type setting proved to be fraught with problems. In 2009, while still at the University of California, Davis, I completed my B.A. thesis on the Heaven’s Gate cult’s mass suicide, masculinity, and media constructions of the normal/abnormal body, and wrote the following as part of my postscript:
…The human body can be—perhaps by necessity—variously embarrassing, bewildering, and beyond control in many ways. Although I have made progress in accepting my various health conditions and dealing with them in the best ways that I know how, the havoc wreaked by these conditions is, at times, incredibly frustrating. The leg that “spazzes” and shakes at inconvenient intervals as a result of mild cerebral palsy, and that I am powerless to stop; the joints, muscles and bones that ache constantly and in different degrees of severity; the fingers that twitch and splay and sometimes press the wrong letters on my laptop keyboard, try as I might to control them; the fibromyalgia’s propensity to make me nearly bedridden at times; my personal feelings of uselessness when–for reasons having to do with extreme pain–I am sometimes unable to complete my academic work on a schedule that resembles a “normal” one for the average college student; my frustration when walking a long distance or climbing up a flight of stairs just seems like too much work; the fact that I am always tired, or hurting, or that I always have fear that my depression will return and do even greater psychic damage than it already has—all of these are things that I deal with on a daily basis, and so of course they affect the work that I do. (63)
Though this is a descriptive passage, looking back, I believe that there is something missing. I can describe the symptoms that I live with daily in the most exacting language possible, but my writing process is such that I usually try to be overly “objective” and “academic” when writing about personal experiences in an academic setting. With cartoons and graphic work, however–a medium in which I tend to feel no such constraints and make no claims to “objectivity” in utilizing it (quite the opposite, in fact)–I have found that I do not feel nearly as much separation from the words that I have written, or from the art that I create. There are ways to represent certain things in art that is exponentially more difficult to do in “straight” writing, and especially academic writing.
The emphasis on an either/or model of theory and practice is of concern to me as well. As Tobin Seibers points out, the current theoretical conception of pain tends to deny, or at least sidestep, the very real and lived physicality of some types of pain: “…pain in current body theory is rarely physical. It is more likely to be based on the pain of guilt or social repression. Society creates pain, but this creation backfires, producing a resource to struggle against society—this is the dominant theoretical conception of pain” (744).
When the pain comes from inside of your body, however, it no longer has a wholly “social” cause that can be easily traced; it is inside you. It is from your body. And, as I hope I have made clear in the graphic novel portion of Nervous Systems, it is— particularly on bad pain days—not a fabulous, transgressive resource that you can then use to fight patriarchy, or capitalism, or Big Pharma, or whatever part of the system happens to be pissing off progressives this week. Sometimes, it confines you to bed, or (horrors) has you relying on medications produced by Big Pharma just to get through the day. Getting up and out into the streets to fight injustice is difficult—sometimes impossible—to do when you are in burning, unending pain that is not caused exclusively by, say, capitalism, but by a nefarious combination of physical issues that are not always within your control, and by the ableism that demands that you should disregard your own pain and fatigue for the good of the progressive “cause,” or because otherwise people will think you are lazy, or that you just aren’t working hard enough to “get better.” Personally, ableism isn’t the only cause of my physical pain and fatigue, but it does not help. One drawback of the pure-theory model, too, is that it tends to remove agency from the people most affected—as Paula Kamen pithily summarizes in her discussion of many feminists’ attitudes toward women’s pain:
In their efforts to counter enemies portraying women as essentially ‘hysterical,’ feminist thinkers have gone too far to the opposite extreme in denying chronic pain’s reality, portraying it as mainly a tool of propaganda against us, a social construct…instead of addressing women’s pain as biologically based, many feminist intellectuals continue to support a seemingly more ‘enlightened’ view: Chronic pain and fatigue are the result of patriarchy (and maybe American capitalism and globalism, too) (168-169).
A pure-theory model also tends to privilege “objectivity” over lived experience without also considering that some of us theorize in order to figure things out, and that theory has to spring from somewhere. When one is writing about personal experience and how it relates to larger social forces, however, objectivity is simply not possible. bell hooks (1994) importantly argues that theory can indeed (and should) come from lived experience: “When our lived experience of theorizing is fundamentally linked to processes of self-recovery, of collective liberation, no gap exists between theory and practice” (61); she cautions, however, that theory “is not inherently healing, liberatory, or revolutionary” (ibid). It can, and has been, used to keep certain people out—people with the “right” qualifications, degrees, and time to study certain theories do, in some sense, have the privilege to be able to pick apart ideas that are, very often, written in a way that makes sense only to people who have these qualifications (hooks 62-63).
Sometimes the opposite happens: questioning theory becomes an exercise in anti-intellectualism, and, as hooks contends, this too contributes to the “false dichotomy between theory and practice” (65). I believe that a lot of theory is useful, interesting, and helpful (I have found Wendell’s, Seibers’, Garland-Thomson’s, and hooks’ work to be both accessible and personally affirming), but even as a “gender studies nerd” who does have some of the “right” qualifications, I have also found much of it to be frustrating, confusing, and weirdly obscuring at times. I often wonder how those who may not have the “correct” qualifications may feel when they come across large walls-of-text which seem specifically designed to speak to people who are not them. I am no supporter of anti-intellectualism or theory-bashing for the sake of it, but on some level, I can (perhaps slightly) imagine how angering it must feel to come across “intelligent” discourse that is meant only for a few, and makes no attempt to reach out to those who might be able to use that theory in their daily lives.
It is for this reason, in part, that I made Nervous Systems a graphic novel. Not only do I excavate and examine portions of my own life and larger cultural/social patterns in order to create theory, but I attempt to make this theory—and some of the theory that came before it, particularly in my use of Wendell, Seibers, and others–accessible by utilizing a format that, while not in wide pedagogical use (yet), has a history as a mass medium. Ironically, in recent years comics and graphic novels have become a new, “hot” form to study in a scholarly way; additionally, “serious” news outlets such as The New York Times have taken notice of the form, and graphic works now regularly appear on many year-end best-of lists. It is, in many ways, beginning to earn the respect of the old- guard literary establishment, despite its background as a “cheap” (and, somewhat hilariously, apparently dangerous, at least during the 1930s) form of entertainment.
Of course, graphic work’s brave new world, so to speak, does not come without caveats. Many successful graphic novels have been created by people who have very similar demographics to those who have traditionally held power in the media—white, heterosexual, able-bodied, middle class or higher men. I think this is changing—albeit slowly—but the still comparative novelty of, for example, women in comics, often gives me pause. People with disabilities working in comics is still a relatively new, and rare, trend. Disabled characters in comics, particularly those produced by mainstream presses, are also a rarity–and even when they are portrayed, they are subject to having important aspects of their stories erased in “reboots.”
I have, I admit, opened myself up to criticism by making myself, certain family members, friends, and other people “characters” in my graphic memoir. The point of this “theoretical memoir” is not to make things up on the fly in order to theorize. The theory here, in which I utilize a form that has not been taken “seriously” in order to explore something—namely, women’s chronic physical pain—that has often not been taken seriously, either: not by society, not by the medical establishment, not by abled people, not by most feminists.
My theory in Nervous Systems comes from a place, or places, of lived experience. As a person in near-constant physical pain, I cannot, as Felly Nkweto Simmonds summarizes, “remain disembodied” when it comes to creating theory (53). The lines of life experience have traced through me, have left their (invisible) marks on my body. The lines of pain have settled into my bones and muscles; those of fatigue shape my sleep and my waking hours. And so I leave lines on the page, first in pencil, then outlined in black ink: words, images, multiple drawings of my scowling face. The reader sees these lines, reads them, interprets them. I hope that these lines, as they exist on the page, make an impression.
